 -Today is Smarter, Braver, Stronger Day in our household. Christopher Robin says it best when encouraging Pooh through a challenging time: “Promise me, Pooh, that you will always remember you are braver than you believe, smarter than you think and stronger than you seem.” That has always been our mantra to push through because it is so very true and it typically isn’t physical strength, but emotional strength. For us we do not label it as World Autism Awareness Day nor Autism Acceptance Day because we are both aware and accepting every day, especially on the hard days. And in honor of this day, today is the last time I will tell this story, because this summer our son will be 18, and then it will be his story to tell. I remember when he was born, an emergency c-section after a failure to descend. The birth was traumatic to say the least and he had the war wounds to prove it. I didn’t get to see him until 5 hours later, but you know what, I remember thinking he was perfect. And he was. I remember the nights where he would wake up screaming and I would instinctively take off his onesie and bounce him back to sleep and the endless trips around the dining room table, rocking him up and down just to get him to settle. We loved how he waved his hands and tapped his foot in the johnny jumper for hours. I remember the distractibility as soon as the cat came in the room when he was feeding and then it would take another 45 minutes to get him to finish. I remember making a cement hand print to put in his room and throwing it away because he couldn’t tolerate the wet texture of the clay. I remember him standing on one foot like a flamingo in the yard because he wouldn’t put both feet down in the grass. I remember him only eating thicker foods and not even touching his 1st birthday cake with tears in both his eyes and mine because I didn’t understand his sensory defensiveness…yet. I remember him getting kicked out of preschool because the school didn’t want any children with behavior problems- that’s why they implemented a behavior plan the third month after we started. They said he was playing with a toy wrong and they didn’t have the time for someone to work with him through transitions from outside to inside. After that, I remember the years of therapy, OT and speech, when my husband would take him weekly without fail. I remember his BSC and TSS come to our home every week to work with him on social skills. I remember when his developmental pediatrician told us his brother would be his best therapist. I remember the day the neighbor started the boat in his backyard after a long winter and startling him where he wouldn’t go outside for three days in fear of the noise. I remember the headphones he wore as he drove around in his play jeep. I remember him talking to and chasing his shadow, wiggling his fingers the whole way. I remember the millions of flaps those little hands, fingers and toes would make as he stimmed off of spinning objects like a fan. I remember hours of tantrums with transitions and bear hugs on the kitchen floor with both of us in a heap of tears. I remember a backyard full of swings, sand, bubbles, chalk, rock walls and anything my OT brain could think of to increase his tolerance to … well, the world. As he got older, I remember the awareness, his awareness to his body and his brain. Why can’t my brain think the right way? Why can’t I talk right? Why do people from elementary school talk to me like I am a child even though I’m in high school? Why is the one thing that still hangs on the stimming when I get excited? Why am I so stupid? And then there was this year…a senior year in high school during a global pandemic that was a challenge for all kids, never mind ours. I remember giving him all the strategies to be successful in school, which he applied, and now the game changed to being online, learning in a whole new way, in a whole new environment, and now those strategies didn’t work. I remember the struggle and heartache as 14 years of executive functioning strategies just went out the window as we had to switch gears. But I also remember the good. Oh, how I remember the good; the successes that may seem so little to some, but are monumental to us. The reason why I am telling this story for one last time. I remember the praises the teachers gave him. “He is so smart.” “If I let him pace, he listens.” “He is so kind.” “He is the sweetest kid I know.” “He is always trying.” And I know for certain he is THE best hugger. I remember being on high honor roll every single school year. I remember the first time he peeled a hard-boiled egg. I remember the first time he wore jeans and a tie. Yup, it’s that simple. I remember the first day he walked out onto the marching band field and watched this sensory defensive, dyspraxic kid buzz into a trumpet and march to near perfection while drums beat behind him and I just looked at him in awe knowing what it took cognitively and physically to make that happen. And then they all won championships! I remember when he got behind the wheel of the car and drove away to his first job. I remember this Christmas when we surprised him with his acceptance letter to the college of his choice. I remember hikes in Acadia climbing ladders stuck in rocks, paddle boarding on a lake, going to rock concerts and feeling the music. I remember watching him grow into a handsome young man and thinking, “we actually did it.” These moments are things I never thought would happen when I heard the words, at 3 years old, “pervasive developmental disorder, most likely of the Asperger’s variant”, not yet known as Autism Spectrum Disorder. The criteria includes social interaction and communication deficits along with repetitive behaviors with criteria in hyper sensitivities, stereotypies, fixations on unusual objects and inflexible adherence to routine. These manifestations still rear their ugly head from time to time, when he is stressed or just being a teenage boy, but I cannot begin to explain how proud and awestruck this mama is of her son as he transitions from high school during a global pandemic and leaves on his way to college in a few short months. And I am thinking, he is perfect, but it is now his story to tell. Excuse me while I get my tissues. There is hope to all of you April 2nd families out there. It may not be the Italy trip we all planned for, but Holland is a pretty cool place too, even 18 years later.
0 Comments
Interoception is a sense within everyone’s body. It lets us know how our bodies feel, especially on the inside. Interoception is the sense that helps us understand when our mouth is dry, when our feet are sweaty, when our hands are warm, when our ears are focused, when our eyes are heavy, when our muscles are tight and when our heart is racing. These sensations can then correlate to an emotion. Pain, hunger, thirst, anxiety, sadness or the need to use the bathroom are examples of the emotional components of interoception.
When you are aware of these sensations, your body helps to determine the essential emotion behind it. Interoception is realizing how your body feels and helps to manage the emotions that follow. For example, if your hands were sweaty, your feet were shaky, your muscles were tight and your heart was racing, this would help you to understand that you might be anxious and need to find comfort. A dry mouth and growling stomach could help you to understand that you are hungry and prompt you to find food. However, this is not always the case! For several individuals, especially those with conditions such as Autism Spectrum Disorder, ADHD, sensory processing disorders, it is difficult to distinguish between all of the feelings. They might notice something happening in their bodies but are unable to describe how it feels. When this happens, they are unable to pin it to an emotion and solve through an appropriate action, like eating to resolve hunger. For example, someone might feel ‘something’ in their stomachs but would have a hard time differentiating if it feels like it is growling, full, empty, tight etc. If this were the case, imagine how difficult it would be to determine if that ‘feeling’ in your body was because you were hungry, full, sick or needing to use the bathroom?!?! So what can be done to help? Research shows that interoception can be improved! Dr. Kelly Malher has created a curriculum for developing mindful self-regulation to improve interoception. Interoception awareness builders are used to incorporate mindfulness techniques with solid visual and sensory experiences. Here at A Rise Above Occupational Therapy Services, we work to improve interoception, despite age or condition. With the training and certification from Dr. Kelly Mahler, we strive to help you understand “how does my body feel?” Social distancing from the COVID-19 spread has given us an amazing opportunity to spend quality time with our families. But you can only play the same board game so many times before fights break out or it just gets boring, right? Therefore, we have compiled a list for you of 25 board games that can be purchased for under $25, many even under $10, to keep you and your family entertained.... because hands on learning and fun is so much better than screen time! Some of them are tried and true, but others you may have not seen or heard of before so we wanted to share. The list doesn't have all of our favorites, but it does cover a wide range of age-appropriateness and skill development. Check out the links for each activity for more details. We have even listed occupational therapy skills that each game works on in the photos below. A Rise Above Occupational Therapy wants you to enjoy this new-found time with your family and develop a new leisure pursuit that you can perform together.... Game Playing! And yes, we have played them all! Check out our list here in alphabetical order: 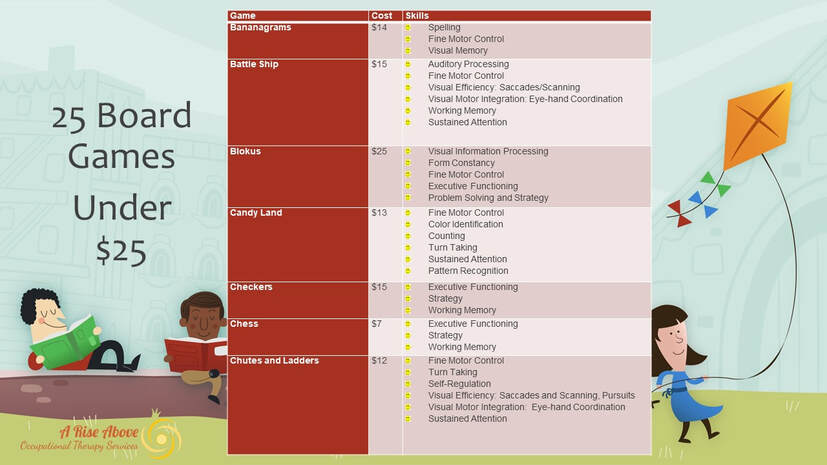 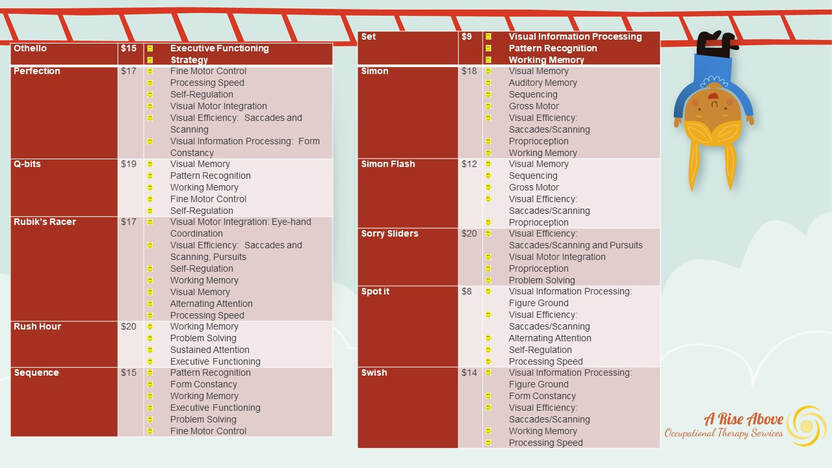 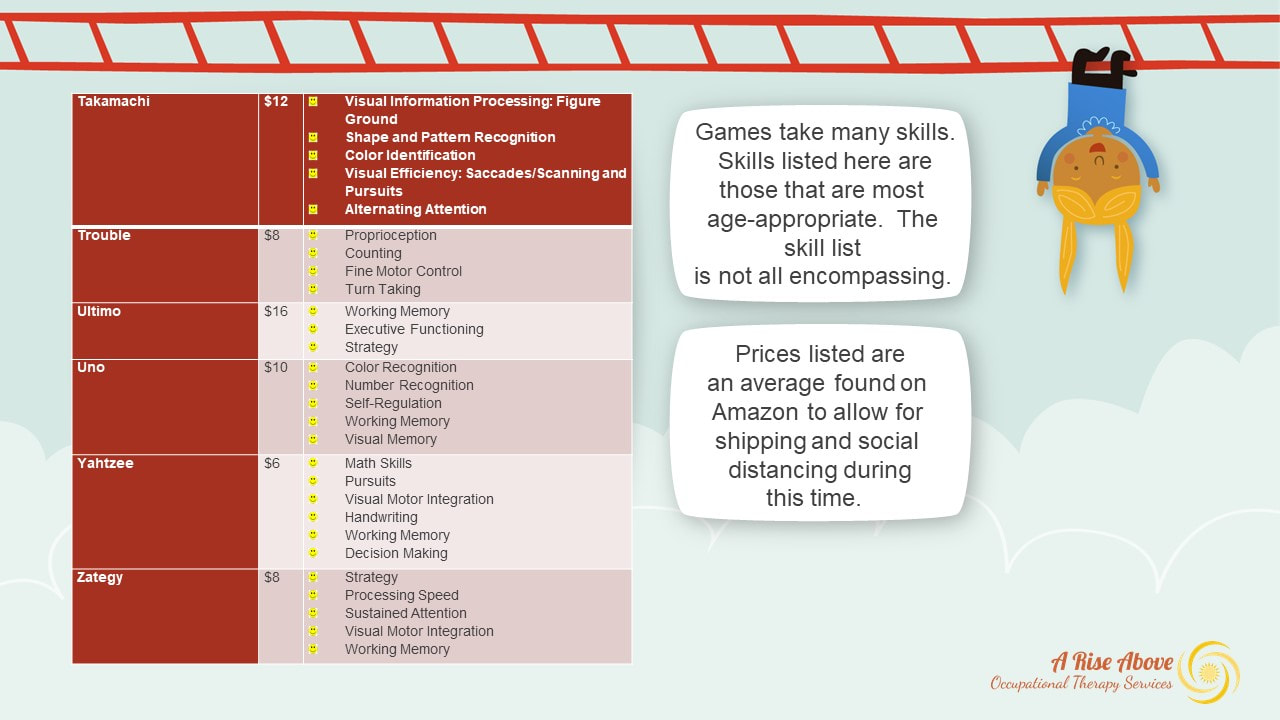 To all the healthcare providers who get screened each and every shift in order to take care of those currently in the hospital, skilled nursing facility, assisted living and the like;
To all the first responders, EMT, Fire, Police who go all in without a question...as always; To the school boards and teachers who are trying to manage their own families and take care of our students now that schools are closed; To public officials who are writing Acts to pass during this pandemic to improve healthcare options and help small businesses who face short to long term closures; To small business owners who are facing the unknown; To those of you who are staying home to flatten the curve; To families who are seeing this as a reset button; To the grocery clerks who are working quickly to get us through the lines and restock the shelves; To those who are immunosuppressed, have diabetes or are over age 60 and may be a little more concerned than the rest of us; To those who have loved ones in nursing homes or hospitals that can't be visited due to restrictions; To those offering help to those in their community either through donating supplies or food or child care; To those who have already been touched by the virus personally and see what it can do to those severely compromised; To those who realize that answers will not be immediate, that recognize that this is a first and everyone is doing the best they can with what they have, day by day, hour by hour, minute by minute....I see you, I thank you, I am you. #ARiseAboveOT -Go big or go home! Bigger is better! We have all heard these sayings and many times they ring true....the last minute of a football game when you are down by three points; when you decide to face your fears and finally go skydiving; when you decide to go back to school after 20 years and change your career. Absolutely! But I have also come to realize that bigger isn't always better....BETTER is better. And here is why that rings true in a private practice therapy setting. 1. You are met with someone who truly believes in what they do. I know that I can help you. I believe in my profession and I believe in my skill set, or I wouldn't have taken the leap into private practice. I left larger networks because it wasn't genuine. I had to meet productivity guidelines and play the games of keeping people in network, not referring to someone who I felt was better skilled to help you, but instead to someone who worked for the same place I did, just because. It shouldn't work that way. I couldn't develop the programs to better serve my patients because it took 3 years to establish. Now, if I want to develop an idea, it happens and it serves you faster! 2. You get to work on YOUR goals. Sure, you may mention what you want to get out of therapy at other places, but do you actually get to work on those things? Does the therapist who is treating 4 patients at a time actually listen and hear what you are saying? Maybe, maybe not. In private practice, we set up your appointment times, not the secretary, so that you are best served. Here, you are seen 90% of the time one-on-one. That means 100% focus on YOU! 3. You get treated by certified therapists here too. Did you know that I'm certified in just as many techniques as therapists who treat at the larger networks? Here are just a few:
4. It's not a gym. For some, they only feel like they are participating in therapy if there is a lot of equipment and technology. And that is ok. But there is much to be said about simple, hands on techniques that focus on performance and skill, rather than fancy equipment and loud gym environments. Concussion Rehab should not take place in an open gym. LSVT BIG should not be performed while treating another person. Hand therapy should not be 4 people sitting around a semi- circular table as the therapist moves down the line from person to person. Occupational Therapy is skilled to look at the whole person, and if your clinician is only looking at your piece or part, know that you deserve more. That's not what OT is. 5. You may actually wind up paying less. If you have a co-insurance, meaning you pay a percentage of each session prior to meeting your deductable, you will wind up paying more for less at big network hospitals. The truth of the matter is, insurance companies reimburse private practice less. Here is an example using round numbers for ease. You are seen for 60 min and have a 25% co-insurance. Private practice gets reimbursed $100, so you would pay $25 for the session. Hospitals get reimbursed $400 for that same hour, doing the same techniques. So now, you pay 25% of that....or $100. Let's read that again. $25 for private practice or $100 for larger networks! Why would you pay more for less quality time? Because they tell you that you have to stay in network....but guess what? You don't. You have the right to seek out any provider you want. They still get updates from us; it's still uploaded to their systems; they can't make you go to them just because they say so. So when it is time to pick a provider, remember that you have choices. Do you want bigger....or BETTER? It's really up to you. And isn't that really what you want in your recovery? #OTCanHelp “I went to the eye doctor and they said my eyes were fine.” As the saying goes, If I had a nickel for every time I heard this. I do hear this a lot, almost weekly, while doing concussion rehab in my practice. So when the patient says my insurance company will only allow vision exams by such and such a doctor, I warn them of this potential outcome before they even go. Yet after the exam, I continue to hear in the clinic, “My vision is blurry; I get a headache from the screen; I can only read for 5 minutes before I get nauseous or a headache”. So now what?! As an OT, my main concern is that these people can’t function because of their symptoms or perform their occupational roles- student, worker, driver, athlete, child, or mother. Over the years, I also got frustrated for these patients who kept getting steered in the wrong direction, so I sought out courses that were taught specifically by eye care specialists and even went back for my clinical doctorate, specializing in vision remediation. This is what I learned:
OT’s are the experts in activity and occupational performance: Occupational therapy distinguishes itself from any other field by analyzing occupations and activities. We look at the person, the occupation, the environment and the performance in order for our clients to be independent. When a child can’t play, we assess why not and address it. When an adult can’t work, we assess why not and address it. We look at the skills needed for that task and compensate for, adapt or restore that missing piece. That is what we do and we are good at it! Many times, the performance skill that is lacking or impaired is related to vision. Adult patients may say, “I get pressure in my temples when I read or think too hard”. With children, they may not be able to verbalize a headache during play, but they may bring an object closer or farther or maybe even not attend to the object at all. This behavior can also indicate a vision problem. Occupational therapists are fortunate because physicians refer to us when there is a problem with activities of daily living, play and fine motor or returning to learn. We are the client’s first line of defense when they can no longer participate in life. That being said, we need to acknowledge that there may be a visual inefficiency causing their problem based on what is seen in our sessions and reported by family feedback. We need to be the referral source to eye care specialists for these patients that we see weekly, BUT we must know who to refer to. OD’s are the experts in vision: To differentiate, an ophthalmologist is a Medical Doctor that specializes in eye care, including the diagnosis, management, and surgery of ocular diseases and disorders (American Academy of Ophthalmology, 2018). The main emphasis is on surgery and prescribing medications for eye disease. However, they spend limited time in their education on the areas of visual efficiency and visual information processing and focus on a single component model of vision that only incorporates the category of visual integrity problems. Optometrists are trained to use the 3-component model of visual integrity, efficiency and information processing (Ciuffreda, Ludlam & Yadav, 2015; Scheiman, 2011). They have a more complete understanding of the use of lenses, prisms, and vision rehabilitation to remediate ocular function, in turn, improving visual and occupational performance. It is important to note that while all optometrists receive this training, only a small percentage practice in this way. I equate these two professions’ relationship to the OT and PT relationship. Let’s take an orthopedic condition, like a hip fracture. A physical therapist may look at the structure of the hip, including the strength and ROM of the hip, pelvis, and back so that the person can get back to walking. They may issue a cane or a walker so that they can move around. Occupational therapists, in turn, will look at the function of the entire person- can they dress themselves with or without adaptive equipment, can they get to the bathroom, can they stand and cook a meal, can they perform leisure pursuits? The same is true for these two eye care professions. Ophthalmologists will look at the structure of the eye including the retina, the optic nerve, while checking for such things as glaucoma or cataracts. They may issue glasses so that the client can see. Optometrists, in turn, will look at the function of the eye- are the eyes converging and working together, are they communicating to the brain to perceive their environment appropriately, are they getting headaches after reading for 5 minutes due to an eye inefficiency? Each profession has a role in serving the client, but they are also specific, resulting in different treatment. In terms of concussion rehabilitation or pediatric therapy, occupational therapists should be referring to those who perform a comprehensive eye exam and acknowledge the dysfunction occupational therapists see during treatment. This means referrals should be made to optometrists; but even within optometry, there is a lack of consensus and uniformity in the way eye examinations are performed. The eye-care professional that occupational therapists chose to refer to should perform the examination using a 3-component model of vision that includes the categories of visual integrity, visual efficiency and visual perceptual deficits that can impact occupational performance. Visual integrity includes the areas of visual acuity, refraction (optics of the eye), and eye health. This area is always examined by both optometrists and ophthalmologists. The visual efficiency category includes accommodation, binocular vision, and eye movements, while visual information processing includes visual spatial, visual analysis and visual motor integration skills (Scheiman, 2011). Whether an eye examination includes all three of these components or just an assessment of visual integrity plays a major role in determining the outcome of the examination and, subsequently, the care provided to the client. These two organizations are a great starting place to find a local expert: The Neuro-Optometric Rehabilitation Association, International (NORA) is an inter-disciplinary group of professionals dedicated to providing patients who have physical or cognitive disabilities as a result of an acquired brain injury with a complete ocular health evaluation and optimum visual rehabilitation education and services to improve their quality of life. https://noravisionrehab.org/ The College of Optometrists in Vision Development (COVD) is a non-profit, international membership association of eye care professionals including optometrists, optometry students, and vision therapists. Established in 1971, COVD provides board certification for optometrists and vision therapists who are prepared to offer state-of-the-art services in: Behavioral and developmental vision care, Vision therapy and Neuro-optometric rehabilitation. These specialized vision care services develop and enhance visual abilities and correct many vision problems in infants, children, and adults. Vision care provided by all COVD members is based on the principle that vision can be developed and changed. https://www.covd.org/ A collaborative effort means the client wins So what does this relationship look like? It has the potential to take many forms. Ideally, it may look like this:
The fields of optometry and occupational therapy are truly kindred spirits. Both professions look at function when serving clients. Both are experts in their own right, but share the ultimate goal of improved occupational performance, symptom free. Both need each other’s expertise to achieve that goal. And ultimately who wins? The client. #OTCanHelp Sources: American Academy of Ophthalmology. (2018). The eye care team. Retrieved from: https://www.aao.org/about/eye-care-team American Occupational Therapy Association. (2014). Occupational therapy practice framework: Domain and process (3rd ed.). American Journal of Occupational Therapy, 68 (Suppl 1), S1-S48. doi: 10.5014/ajot.2014.682006 American Occupational Therapy Association. (2014). Scope of practice. American Journal of Occupational Therapy, 68 (Suppl 3), S34-S40. doi: 10.5014/ajot.2014.686S04 Ciuffreda, K. J., Ludlam, D. P., & Yadav, N. K. (2015). Conceptual model pyramid of optometric care in mild traumatic brain injury (mTBI): A perspective. Vision Development and Rehabilitation, 2, 105-108. Scheiman, M. (2011). Understanding and managing vision deficits: A guide for occupational therapists (3rd ed.). Thorofare NJ: Slack, Inc. A new year brings new experiences, new activities, and you guessed it, NEW OCCUPATIONS. That goes for me as well. I truly believe that education and program development are the cornerstones of giving good care to those we serve. Everyday is a new opportunity to rethink out of the box and resolve ourselves to improving our skill set. This year I am fortunate enough to be able to offer that education to our state professional organization (POTA) members regarding vision dysfunction's impact on occupational performance. I hope this forum will provide an arena for discussion and education for others, as well as myself, in order to move our profession forward and continue my own growth and understanding. I am posting this blog here as well because it is important to know who is treating you, what's the backstory, and....what is she up to now? ____________________________________________________________________________________________________ ...We wanted to start the group off by introducing ourselves and giving you a brief history of why we asked for this network to be initiated within the Commission on Practice sector of POTA. I have been an occupational therapist for 18 years and, in that time, have worked primarily with adults and geriatrics in various settings. My love revolves around neuro rehab, including strokes, MS, Parkinson’s and most recently concussions. As concussion rehab has come to the forefront over the last several years, my interest became locked in on visual dysfunctions and symptoms that were common place for those who sustained a concussion. In 2013, I took my first vision continuing ed course, “From Eyesight to Insight”, co-taught by Mary Kawar, OTR, of astronaut training fame, and Carl Hillier, OD, FCOVD, creator of the multimatrix game. It was geared towards pediatric therapists but I thought that it could definitely apply to adult neurological rehab as well, so I took a chance and took the course. Little did I know at the time how influential these two would be on my understanding of visual screening going forward. I took their information and started to apply it to my practice. So now I had this awesome toolkit on how to screen for visual dysfunction, but no one to refer to. Within our network there was no one who acknowledged the need for vision remediation and the closest optometrist who did was 50 minutes away in another state. I tried to work with an ophthalmologist 2 blocks away who said to me upon meeting, “You don’t believe in that vision therapy stuff do you?”, and handed me the American Academy of Ophthalmology’s position statement from 1999 that stated there was no research and it didn’t work. This was 2014. I was so frustrated having identified a huge area of dysfunction that no one was addressing, and I, as an OT, couldn’t address, as prisms and lenses were out of my scope of practice to assist with blurred and double vision. Fast forward to 2016. My supervisor, knowing I had an interest in vision, sent me a link to another pediatric course, taught by Mitch Scheiman, OD, PhD, FCOVD. It was here that I learned of the new clinical OTD that was being offered at Salus University. My mother, Maxine, had just passed away 6 weeks prior to this course, my dad was most likely going to be moving in with us from CT…how on earth could I even entertain getting my doctorate just because I liked vision and identified its impact on occupational performance? At the end of the day, Dr. Scheiman mentioned a story about his wife, who was an OT…. her name? Maxine. I took it as a sign to follow my instinct and sign up. After 16 years of practice, I was back in school and learning from the best. I was honored to have the support of Dr. Scheiman as my mentor, who has over 200 published articles regarding vision dysfunction and remediation. After explaining my frustrations to him both from an OT standpoint with every therapist having a different understanding of skills and role, and frustrated with the eye-care profession after hearing for the millionth time, “Their eye health is fine”, I developed my capstone. It was a survey that I created, sent to therapists in the most densely populated OT licensed states, regarding “Concussion-related vision disorder practice patterns in occupational therapy”. Questions revolved around screening technique knowledge, treatment practice patterns, referral patterns, certifications and continuing ed, scope of practice beliefs, frames of references and what, in fact, is OT's role, if any. And the results that I got were proof positive that something needed to be done! Data from this study suggested the need for the following changes in occupational therapy practice:
Having presented my poster this past Fall at the American Academy of Optometry in San Antonio, and being accepted to present this April at AOTA in New Orleans, I know that my research is important not only to me, but at least two other professions. I look forward to providing you with evidence-based practice and information that will help you help your patients when they demonstrate dysfunction with visual acuity, visual efficiency and visual perceptual skills. Let’s move the profession forward. Cheers! #OTCanHelp   It's that time of year again when we all look at our lives and determine what it is we want to improve upon. Ok, let's be honest. Resolutions typically revolve around what we don't like about ourselves.... our diet, our temperament, our lack of exercise or not being the best person we know we can be. I know mine usually do. And by the end of January, if I'm lucky, they have fallen by the wayside and put back on the list for next year.
So why aren't we successful in keeping these promises to ourselves, the most important person in our lives? While reflecting on why mine usually fail, I had a revelation. Resolutions are synonymous with occupations and life roles and routines. Funny, as it's the basis of the field of occupational therapy and here I am, failing at it every year! So what if for 2019 I pick an occupation I want to work on and start to adapt that to how I want it to look? Occupations are everything we do in a day... eating, exercising, working, seeking out leisure like crafts, woodworking, gardening. Hey look, resolution material! Here's what I'm thinking: for example, let's look at the resolution of improving diet and nutrition. To achieve this resolution, we need to create healthier meals, whatever that looks like (sugar detox, keto, paid for diet plans). This goal involves making menus for the week, grocery shopping, meal preparation and clean up, as well as hydration and exercise. That in and of itself seems daunting regarding changing routines in ALL of those areas. No wonder I have failed. For each one of those tasks it takes 21 days to create a habit or routine! That's where the OT in me had an ah-ha moment, maybe long over due. What if I break down the overall occupation of maintaining a healthy diet (dream) into each component activity (goal) so that I can succeed in little steps, one task at a time each month (plan)? Maybe in January I could focus on buying more fruits and veggies (action), cutting them up for the week and making sure that I eat them everyday for lunch instead of throwing them out in a week because I forgot about them. In February I could focus on drinking more water and eating a healthy breakfast BEFORE work, in addition to my January achievements of fruits and veggies for lunch. March could bring a week at a time of meal planning, with grocery shopping on certain days making a concrete routine and habit within my role as wife and mother. All of a sudden, I have made diet changes to 3 meals a day over a period of time. Now, this resolution of improving diet and nutrition doesn't seem as daunting compared to my usual "January 1st all this must change or bust". It is truly looking more like a life change. And this life change can be my new reality. How simple to use this new perspective...and why did it take me so long to realize this step by step approach when it's what I preach everyday?! And so to you I say, Happy 2019 a few days early. Let us all start January with a simple occupation that you want to change. Break it down into smaller pieces and spread it out over time to make it more routine, rather than jumping in gang busters. You may be surprised if by June you are still hanging onto your "resolution" and creating a new reality that's all about YOU! CHEERS! I'll keep you posted on mine.
|
Author:
|


 RSS Feed
RSS Feed
Hours of OperationMonday 8 am- 6 pm
Tuesday 8 am -6 pm Wednesday 8 am-6 pm Thursday 8 am-5 pm Friday 8 am - 12 pm Sat - Sun: Closed |

Services:
Neuro Rehab Pediatrics Concussion Rehab Vision Remediation Telehealth Interactive Metronome Interocpetion |
Contact Information Phone: 484-215-4690
Fax: 610-419-0312 Email: [email protected] NOW: ONE LARGER LOCATION 2380 Schoenersville Road Bethlehem, PA 18017 |
Site powered by Weebly. Managed by FreeLogoServices.com
|
|
|